
The MIST Model in Action
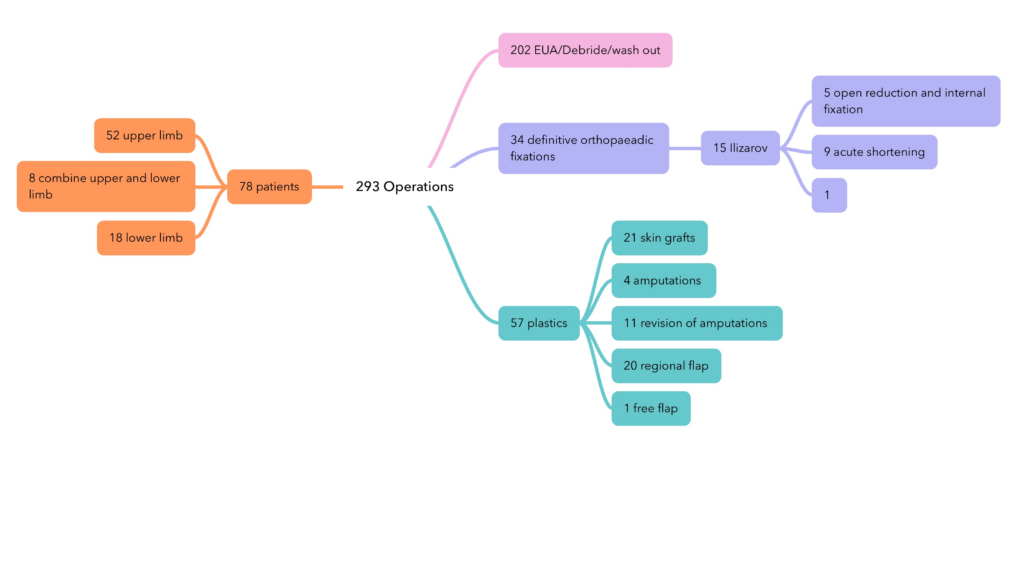
The flow chart depicts the sample of patients and their respective operations performed over a 12 day period. The numbers and flow relate to this specific cohort of patients but provides a visual guide to what is achievable when planned correctly.
The MIST team averaged 24 operations per day split to concurrently operate in two adjacent theatres.
Further details can be found in the published paper: Experiences of a multidisciplinary surgical team. Prehosp Disaster Med 2010;25(4):361–367
Preparing for the MIST Model. Step 1: the core team
Having experienced, capable, hand-picked team members with known characteristics able to be deployed at short notice, MIST selects high calibre staff from around the world.
Twelve teams are on stand-by. Each core team consists of an orthopaedic surgeon, plastic surgeon, anaesthetist and operating department practitioner. Depending on the situation MIST can reduce or expand the team accordingly by paring down or utilising additional staff such as scrub nurses, physiotherapists etc.


Initiating the MIST Model Step 2: partnering, funding and access
Project funding is generally from non-governmental organisations(NGOs) and governments who understand the expertise and 20-year track record of MIST and it’s capabilities in limb recon. A government or NGO may request MIST’s assistance based on a pre-agreed package of support. MIST ensures that the funding will deliver the required care, services and outcomes desirable in each situation.
Access, transportation of members and equipment, accomodation and subsistence are required in each jurisdiction and according to local laws.
Step 3: local considerations
Functioning hospitals and theatres are required whether an existing dedicated facility, re-purposed facility or field hospital and will have been identified prior to arrival.
Staff: available local staff are identified and brought under the wing of MIST. Any deficiencies can be addressed through mentoring and education.
Patients: initial screening for suitability, operations planned, post-operative recovery and rehabilitation planned, ongoing support and follow-up.


Step 4: Operating protocols[and follow-up]
In emergency situations there are two distinct areas: emergency/trauma surgery and elective. Emergency surgery is often life or limb, wheras elective surgery is pre-planed and follows the in initial patient stabilisation phase.
In both scenarios careful and timely follow-up focus on the best outcomes for patients. Limb reconstruction utilising the Ilizarov frame requires frequent checks and adjustments to guide the bone growth.
Step 5: Support and Self-Sufficiency
MIST uses trained local staff to monitor patients directly and also remote support utilising surgeons and past patients to assist with ongoing guidance and support.
Repeat visits to limb reconstruction units to update and discuss cases and learning with local staff at pre-determined intervals always working towards self-sufficiency.

